INTRODUCTION
PCOS is a heterogenous condition that affects women of reproductive age. Although the underlying cause of PCOS is thought to be an increased LH: FSH ratio, insulin resistance is also implicated in the pathogenesis of disease.
DIAGNOSIS & PHENOTYPES
Diagnosis of PCOS is according to the Rotterdam criteria: at least two out of three of hyperandrogenism, ovulatory dysfunction or polycystic ovaries, with exclusion of related reproductive disorders.
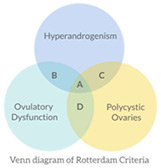
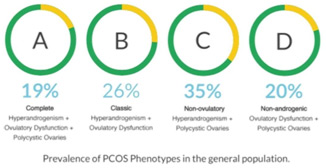
Phenotypes A & B together are often referred to as Classic PCOS and make up 45% of disease in the general population. Women with Classic PCOS appear to be more hirsute and obese, have worse menstrual irregularity and are more likely to be insulin resistant. Insulin resistance means a higher risk of future metabolic syndrome and a reduced chance of achieving a live birth.
PATHOPHYSIOLOGY
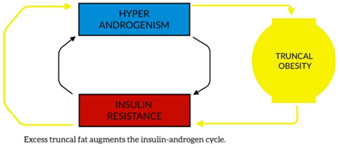
It is important to remember that insulin resistance is tissue selective in PCOS women. Although skeletal muscle, adipose tissue and liver lose their sensitivity to insulin, adrenal glands and ovaries remain sensitive. In order to overcome resistance in peripheral tissues the pancreas increases insulin production and the still sensitive ovaries and adrenals receive a relatively high dose.
Hyperinsulinaemia increases free androgens:
- increased ovarian and adrenal production of androgens
- reduced Sex Hormone Binding Globulin production in the liver.
Hyperandrogenism in turn exacerbates insulin resistance:
- reduced number of GLUT-4 receptors
- reduced insulin degradation in the liver and
- decreased skeletal muscle insulin sensitivity.
Thus, a vicious cycle occurs between androgens and insulin. Unfortunately, hyperandrogenism also has the additional effect of increasing fat deposition in the truncal zone. As excess fat accumulates in this area so does overall degree of insulin resistance which is like pouring fuel on a fire.
WEIGHT LOSS MANAGEMENT
- Weight loss of 5-10% reduces circulating androgens improving menstrual regularity and fertility.
- Metformin increases insulin sensitivity while inhibiting ovarian androgen production.
- In 2019, Cochrane reported that metformin use in women with PCOS has insulin lowering effects, a potential benefit in live birth rate and no conclusive effect on BMI.
- Meta-analyses of GLP-1 agonists (Liraglutide, Saxenda) show they appear to be more beneficial for weight loss and insulin resistance compared to metformin however data quality is low.
- A recent meta-analysis compared metformin to bariatric surgery in women with PCOS and obesity, 10 studies with 587 patients were included (Chang et al, J Gastrointest Surg, 2021).
- Metformin increased the likelihood of pregnancy compared to placebo however bariatric surgery improved fertility more than metformin therapy Those who underwent bariatric surgery were more than twice as likely to become pregnant than those treated with metformin 34.9% vs 17.1% (p = 0.026).
- Contraceptive counselling occurs prior to surgery as fast resolution of ovulatory dysfunction leads to high risk of unplanned pregnancy during the rapid weight loss phase.